What is the Gendered Health Pathway?
The Gendered Health Pathway is an analytical construct delineating the trajectory from risk factor exposure and disease prevalence to the ultimate health outcome, bringing together different stages of the care cascade. In this project, we gathered data, stratified by sex and age at each step of this pathway. It is important to acknowledge that our data, derived from diverse sources, reflects population-level phenomena and is not individually attributable along the pathway.
Identifying data sources for the Gendered Health Pathway
Global data on certain health pathway components, such as disease prevalence and final health outcomes, are widely available from multiple sources. However, a notable scarcity exists in global-level data regarding disease-specific care pathway. We conducted a comprehensive scoping exercise, focusing on disease-specific care pathway. Our criteria included disaggregation by sex and age, along with information covering at least three cascade steps: diagnosis, treatment, and control. We searched for data on COPD, depression, diabetes, HIV, hypercholesterol, hypertension, lung cancer, and tuberculosis and found suitable data for three conditions: diabetes, HIV, and hypertension.
Data for hypertension and HIV care cascades were extracted from global-level, harmonized datasets provided by NCD-RisC and UNAIDS, respectively. For diabetes, lacking a collective dataset on the cascade, we analyzed country-level data from WHO’s STEPwise Approach to NCD Risk Factor Surveillance surveys (“WHO STEPS”) to estimate the diabetes care cascade by sex and age, for the country-year combinations for which the surveys are available.
Upon identifying conditions with a complete care pathway data, we completed the health pathway by incorporating data on relevant risk factors (e.g., smoking, alcohol, obesity), prevalence and disease-specific final health outcomes (death rates) from the Institute for Health Metrics and Evaluation (IHME). To ensure consistency across different data sources, we harmonized age groups, maintaining uniformity throughout the pathway. To do so, when necessary, we aggregated smaller age groups data into wider, standardised age groups, using the IHME age-specific population.
Risk factor and mortality data for all three conditions are available for 204 countries from IHME. Prevalence data for hypertension and diabetes are available for 200 countries from NCD-RisC. IHME population data is not available for French Polynesia so rates could not be calculated. We removed an additional seven territories from the dataset that are not sovereign states as recognised by the United Nations. Thus, in total 192 countries are visualised in the dataset.
Care pathway data is available for 192 countries for hypertension, 76 countries for HIV and 39 countries for diabetes.
We are grateful to colleagues at IHME, NCD-RisC, UNAIDS and WHO for their collaboration.
Hypertension Pathways Data Sources
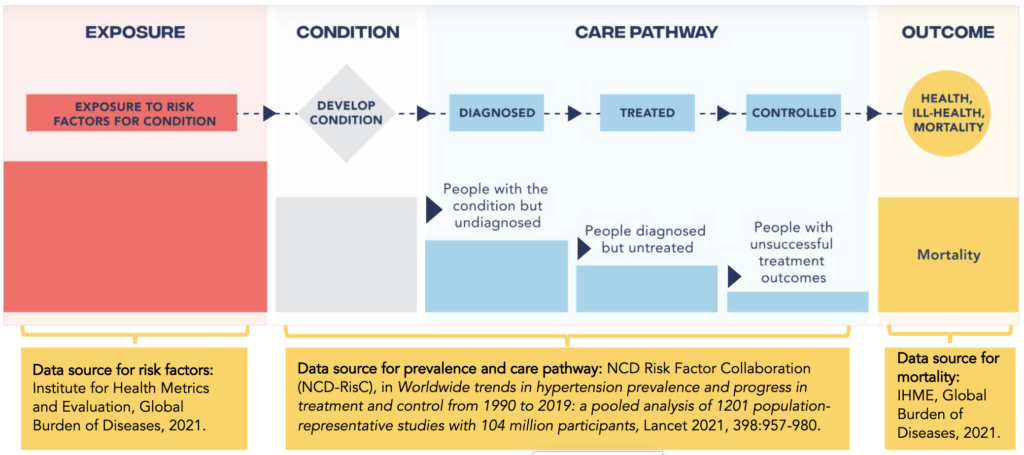
IHME supplied unpublished data on primary hypertension risk factors from the Global Burden of Diseases Study 2021. The Global Burden of Diseases Study was also the source for the final health outcome, expressed as country-specific mortality rates disaggregated by sex and age.
NCD-RisC contributed hypertension prevalence and care pathway data, detailed here Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants Lancet 2021, 398:957-980.
Figure. Data sources
Diabetes Pathways Data Sources
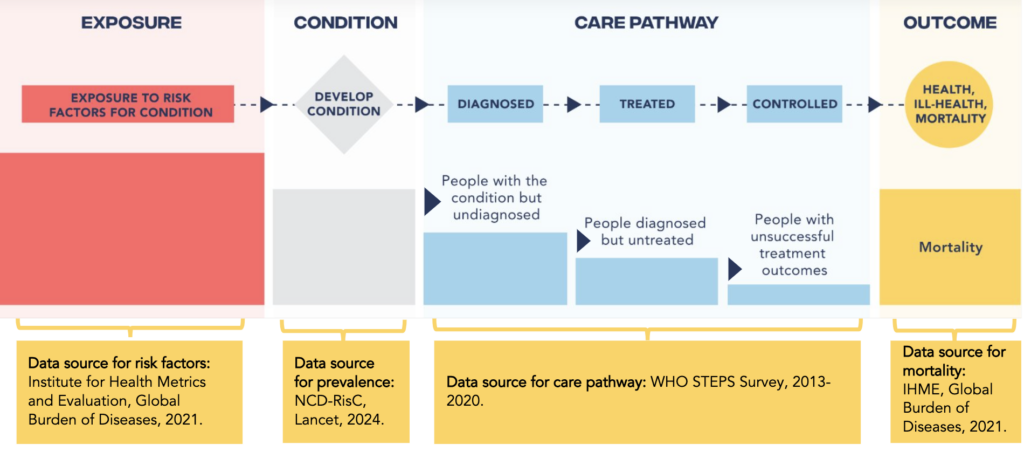
IHME supplied unpublished data on the prevalence of primary diabetes risk factors from the Global Burden of Diseases Study 2021. Data on diabetes death rates were also sourced from The Global Burden of Diseases Study 2021.
Diabetes prevalence data is from Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. Published online 13 Nov 2024. Data can be downloaded here: https://www.ncdrisc.org/data-downloads-diabetes.html
Diabetes care pathway data were derived from WHO STEPS surveys, with analysis conducted for 39 countries post-2013, following the methodology outlined in Manne-Goehler J, Geldsetzer P, Agoudavi K, Andall-Brereton G, Aryal KK, Bicaba BW, Bovet P, Brian G, Dorobantu M, Gathecha G, Singh Gurung M. Health system performance for people with diabetes in 28 low-and middle-income countries: a cross-sectional study of nationally representative surveys. PLoS medicine. 2019 Mar 1;16(3):e1002751.
For the diabetes care pathway, we restricted our analysis to surveys between 2013-2020 and selected the latest year available for countries, which included only 39 countries, by age groups 30-44, 45-59, and 60-79. Diabetes cascade data is not from one year only.
Figure. Data sources
HIV Pathways Data Sources
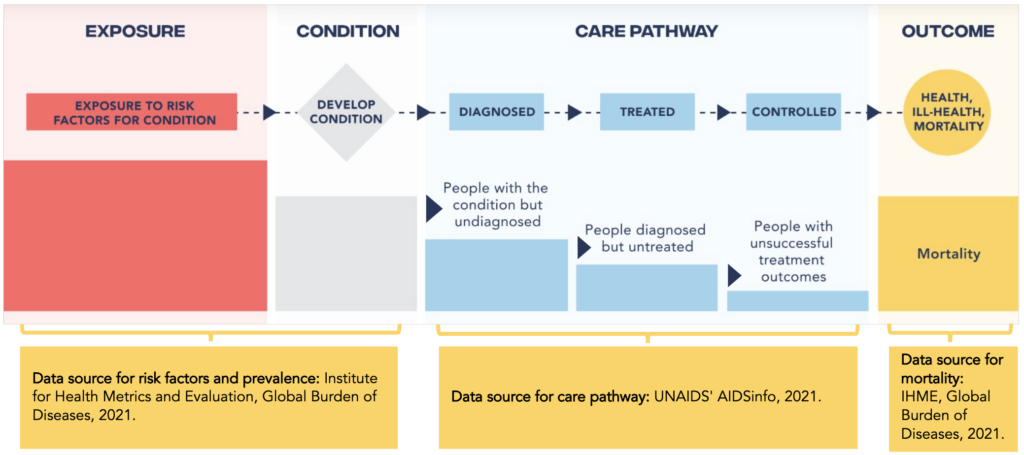
IHME supplied unpublished data on the prevalence of primary HIV risk factors from the Global Burden of Diseases Study 2021. Data on HIV prevalence and death rates were also sourced from The Global Burden of Diseases Study 2021.
UNAIDS’ AIDSinfo 2021 was the primary source for data for the HIV care pathway. Comprehensive details on data can be found at this link aidsinfo.unaids.org. Detailed methods can be found in the Annex on Methods (page 350) of the UNAIDS Global AIDS Update, 2022.
Figure. Data sources
Limitations and challenges
Remarkably, there is a dearth of published analyses and available care cascade data disaggregated by age and sex/gender. Tuberculosis posed a surprising challenge, with a lack of age and sex-disaggregated care pathway data in both primary datasets and published literature.
Compiling a comprehensive set of global-level risk factor data disaggregated by sex and age across multiple countries proved challenging as well. IHME’s Global Burden of Disease project emerged as the only data source offering comprehensive (modeled) global level data on risk factor prevalence by sex and age. We are grateful to colleagues at IHME for providing unpublished data on sex- and age-disaggregated risk factor prevalence.
Acknowledgements
This collaborative initiative is part of a larger programme of work at GH5050 to contribute knowledge on the relationship between gender and health and drive action for more gender-equitable and healthy societies.
Many thanks to Angela Chang and Virginia Zarulli for their leadership in the methodological development of the health pathway, to Alessandro Feraldi for his support in collating the data, to SOAK Digital for the design of the visualisation tool, to Silver District for the development of this site, and to Neo for their close engagement in shaping and communicating this work.